Speaker Series – Episode 7 Summary
In this episode of our Speaker Series, we dive into the world of science to understand Guillain-Barré Syndrome (GBS) and Chronic Inflammatory Demyelinating Polyneuropathy (CIDP) from our Benson Fellowship Awardees Dr. Elba Pascual Goñi MD, PhD, Ruth Huizinga, PhD.
Introductions and basis of their research
Dr. Elba Pascual Goñi: Dr. Pascual is a clinical neurologist at the Hospital of Santa Creu I Sant Pau in Barcelona, Spain. In 2021, she finished her PhD in autoantibodies in CIDP and in 2022 she was awarded the Benson Fellowship. Titled “Biomarkers in the Diagnosis and Follow-Up of CIDP”, her research consists of three parts: research of new autoantibodies, validation of new biomarkers in CIDP, specifically filament levels, and validation of new wearable biomechanics technology to monitor gait and clinical status in CIDP patients.
Dr. Ruth Huizinga: Dr. Huizinga is the foundation’s first Benson Fellowship Awardee in 2014 and is now a biomedical scientist at Erasmus in Rotterdam, Netherlands. Her research includes how the immune system responds to microbes and activation of immune cells in the blood of GBS patients.
Dr. Janev Fehmi: Dr. Fehmi is a trained neurologist whose research consists of looking at the clinical characteristics of a group of patients with immune mediated neuropathies like CIDP and GBS, but were found to have antibodies targeting specific parts of the peripheral nerve called the Node of Ranvier (they are now termed ‘Autoimmune Nodopathies’). In addition, she explores broad mechanisms by which these antibodies were likely to cause damage to the nerve.
What is a Biomarker and why would it be important to the GBSCIDP community?
Dr. Pascual: A molecule, gene or characteristics with a particular pathological or physiological process for disease to be identified; antibodies are a prime example of biomarkers.
Dr. Pascual is investigating a new biomarker by monitoring neurofilaments or, proteins from the skeleton of nerves that is released to the blood when there is damage to the adipose axon of neurons.
These neurofilaments can be observed with a simple blood test and can be used to monitor disease progression and even disease diagnosis.
What are Antibodies?
Dr. Huizinga: An antibody is a Y-shaped molecule with 2 arms that attach to microbes. if an antibody bonds well to another microbe, it can neutralize the pathogen in a bacteria or virus. Each antibody differs depending on the end of its arms as they affect its ability to bond with certain microbes.
In patients with GBS and CIDP, antibodies target certain molecules in the nerves that weaken the nervous and immune system.
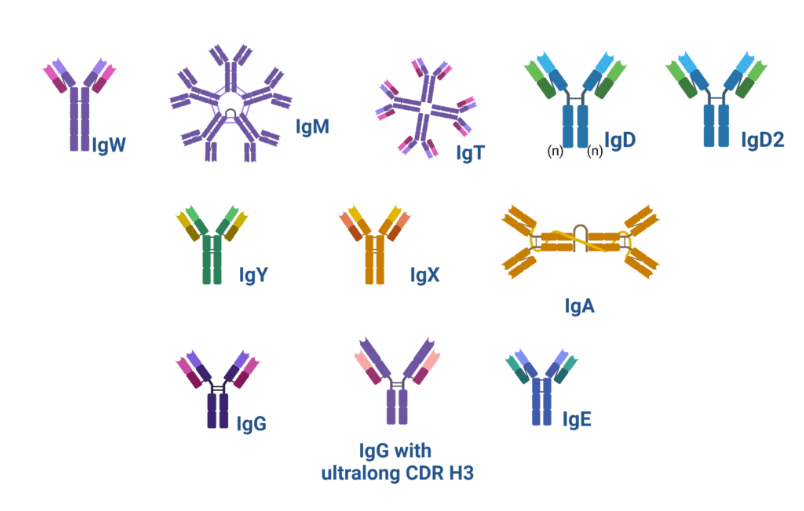
*Picture from María Gerpe, PhD at Rapid Novor
Can you explain the difference between basic research and clinical research?
Dr. Pascual: Clinical Research is research that involves patients and data collections like blood samples to try to understand a disease to develop new therapies. There are different types of clinical trials such as natural history studies that help scientists understand the history of different diseases.
Dr. Huizinga: Basic Research is research with the goal of understanding a natural process such as how molecules work, how cells communicate with each other, and how the body is affected. Basic research does not have a goal of finding a new therapy or treatment.
IGOS is a global study of thousands of GBS patients focused on GBS’s electrophysiological data. Learn more about IGOS here.
INCBase is a database for CIDP patient that is still actively collecting samples for research. Learn more about INCBase here.
What role does each type of research play in improving patient lives?
Dr. Fehmi: My research is based on a small cohort of patients, but has significant implications for the wider group of those with immune mediated neuropathies. Because we believe a large proportion of patients have an antibody driven disease (even if we cannot find the specific antibody), this group of Autoimmune Nodopathy patients serve as a representation of what might be happening in at least some of these other patients. More importantly, they seem to have a specific clinical presentation that makes them stand out, and they don’t respond as well to the standard treatments we have for GBS and CIDP (like IVIg, Plasma Exchange and steroids). They have responded very well to other immune therapies, such as Rituximab, which specifically target cells making antibodies. This finding opens the doors to all those patients who do not present typically or respond well to current treatments and offers a more personalized approach to diagnosing and treating patients with peripheral neuropathies.
What inspired you to pursue this question you are trying to understand with this study?
Dr. Huizinga: I’m a really curious person. So, I want to understand how things work. Just before the Benson Fellowship, we did a study in which we investigated immune responses to Campylobacter. There, we found increased immune responses in patients with GBS. This made us wonder if it could also be applied to other pathogens like viruses, or whether it was more limited to Campylobacter. And of course, you talk to people, your mentor, your supervisors, etc. So, along the way, things will shape more into a proposal. But I think it’s more of the curiosity that drives me.
Dr. Pascual: I am also very curious. I guess this is something common in researchers. So, in the case of my research project, I get the inspiration in the clinic when I see patients with CIDP and also with my mentor, Dr. Luis Querol. We are aware that patients diagnosed with CIDP are very heterogeneous. They have different symptoms, different evolution and different response to therapies. So, we believe that in the CIDP syndrome, there are different subsets of patients that can be better classified to understand the mechanisms that are causing the disease. So, the other problem that we have in the clinical practice is the monitoring of patients to see the progression and the evolution. The response to therapies is not very objective at the moment because we don’t have a biomarker that indicated the status of one’s myelin and axons. We need more objective outcomes. So for all these reasons, we think that investigating the biomarkers and using new wearable technologies may help to better monitor patients in the clinical routine.
Dr. Fehmi: I want to become a sub specialist in peripheral nerve disorders. This group of patients with autoimmune neuropathies represents a very treatable group of patients. Without this, research would have otherwise been considered poorly responsive to treatment and potentially become very disabled.
Are there any unmet needs that you would like to discuss and bring to our audience that you see in this community?
Dr. Huizinga: What makes me curious is the diversity in recovery time between patients with GBS or CIDP: some recover fast and others take much longer to recover. For example, certain patients may have more damage to the myelin that wraps around the nerve fibers whereas some have more neuronal damage or axonal damage. We have been successful at isolating an antibody in both GBS and CIDP patients, but we don’t understand why. Now we need to really know about what the antibody binds to and why it causes damage to the myelin.
How does your research affect people’s lives?
Dr. Pascual: As we monitor the blood in patients we can better treat our patients because we are able to see when serum neurofilaments are active. We can use this data to change one’s therapy or even stop therapy if we observe that their neurofilaments are inactive. In the future we hope to discover new antibodies and mechanisms that cause disease and help decide which therapy is the most useful.
Dr. Huizinga: I hope that we will learn more about the mechanisms that cause these diseases to improve diagnosis and offer more strategies for treatment.
Dr. Fehmi: It offers a new avenue into understanding how and why their disease is causing damage to their nerves, and provides a more accurate prognosis of what the future looks like. It also offers a potential new and more effective treatment, which has not been widely available for decades in the field of GBS and CIDP.
Does your research have a global impact?
Dr. Fehmi: Autoimmune and antibody-mediated diseases are an expanding field of medicine, especially with the advent of more specific and understood immunomodulatory therapies. This research should promote our desire to implement an earlier and more specific diagnosis, and a more targeted treatmentfor patients who are not responding in the typical way. I think this applies globally, setting an example for a personalized approach, and understanding the exact mechanisms of pathology in individual patients.
What would be the next step in your research?
Dr. Pascual: If we find these biomarkers to be useful, it will be continuously tested, and then implemented into clinical practice. There are still some biomarkers that need more research because we are looking at the filament levels that are informing us about the axons in CIDP. We need a biomarker that informs us about the myelin status because some patients with CIDP will have normal serums and filament levels, but have inflammation on their myelin. Therefore, we are looking for a myelin biomarker.
Dr. Huizinga: We are focused on isolating more antibodies from patients with more axonal subtypes and patients with Autoimmune Nodopathies. It is important for us to compare the same antibodies in different patients, especially when they have other autoimmune conditions.
Dr. Fehmi: For me one of the most interesting aspects of doing this research in Oxford is the development of growing live, partially human peripheral nerves from stem cells and applying the patients antibodies to it to assess how they might cause injury. This is a unique and invaluable technique and I would like to utilize it further. With advanced imaging techniques, I think modifying these cultures and seeing what happens in different conditions when individual patients blood and antibodies are added would provide great insight. We need more patients to be recruited to research studies in order to do this effectively. I also think because this group of patients is quite small, we need to collaborate more with international partners and present larger cohorts of patients.
Do either of you use AI?
Dr. Huizinga: Not yet, but it holds a lot of promise and is worth investing in.
Dr. Pascual: We are currently using AI. We are collaborating with engineers in their study of the wearable biomechanical technology and are collecting data from different sensors that patients wear in the legs and shoes. We receive a lot of data from the angles and the vertical force of the feet so all this data needs to be processed with AI. We have a team of engineers that are analyzing all this data. So yes, I think that AI is the future.
For Dr. Pascual, is there a positive correlation between serum neurofilament protein levels and disease severity?
Dr. Pascual: When we talk about serum neurofilament levels we are looking at the axonal damage of the peripheral nerves. So we know that in certain diseases such as GBS, we find very elevated levels of these biomarkers in the acute phase of the disease. When weeks and months go by the patient recovers and these levels slowly normalize. This is very clear in GBS and proves it’s a very acute disease.
We also know that in some chronic neuropathies, like autoimmune neuropathies, this happens. During the acute phase of the disease, patients have elevated levels, and these levels correlate with disease severity. What we don’t know yet is if this also happens in CIDP patients, which is why we are studying this.
Is there any research to better understand why IVIg is an effective treatment?
Dr. Huizinga: Immunoglobulin competes with pathogenic antibodies to block or reduce its effects faster then normal. There are many other regulation mechanisms that make it hard to pinpoint which mechanisms help flag the detrimental effect for IVIg to compete with.
We did a study of CIDP genetic variants to understand why some patients did not respond to IVIg. Although it is far from being used clinically, there are some genetic differences between patients that could help explain this unresponsiveness to IVIg.
Will any of this research have the potential of neuro-restorative outcomes that repair the myelin around the peripheral nerves?
Dr. Pascual: There are no myelin restorative therapies that are effective at the moment, but there are multiple sclerosis studies on the central nervous system. There were some clinical trials investigating this, but the drugs were negative and ineffective.
Dr. Huizinga: We know that some parts of the body can regenerate and luckily symptoms only affect the peripheral nervous system. Yet, since nerves are long and span all the way to your fingers, it takes a long time. There needs to be more understanding of myelin regeneration, but there also is a need to prevent axons from degenerating. So in that respect, the neurofilament Elba is referring to is important in preventing long-term deficits caused by this axonal degeneration.
How can patients get involved?
Dr. Fehmi: At the front door they can ask their physician to check whether there are any trials or research studies they may be eligible for. Otherwise, I think looking on websites such as ours can often sign post to possible research studies.
Can a biomarker help shorten the long diagnosis journey for CIDP?
Dr. Pascual: In essence, yes but we need different types of biomarkers and antibodies to fully improve the diagnosis journey. In the past, patients diagnosed with CIDP have been tested and found other antibodies that are not a biomarker to CIDP which concluded that they had a different disease such as Autoimmune Nodopathy. Therefore, we need multiple biomarkers to make sure that we are positive some has CIDP and not another autoimmune disease.
What is the reason for nerve damage being so asymmetrical, especially in CIDP or MMN?
Dr. Huizinga: These conditions are autoimmune, so we know that inflammation in nerves can be patchy, which results in only one limb being affected versus a symmetrical presentation
Where can we find more about your research?
Dr. Pascual: We do not have any publications but we are starting to present our research at the next Peripheral Nerve Society conference. The best way to find out more is by attending more of the foundation’s events.
Dr. Huizinga: Scientific journals and publications are free on online and you can find more of my research with IGOS here.
Dr. Fehmi: My research can be found by searching for my name, Janev Fehmi, on a publication database such as ‘PubMed’. It is also available through links on my supervisors, Associate Professor Simon Rinaldi, Oxford University, webpage. He is leading research in this field in the UK.
Final Thoughts from Dr. Huizinga and Dr. Fehmi
People always want to know the overall status
Dr. Huizinga: It takes a lot of work to get from the idea, collect data, do the measurements, analyze and reanalyze. Money is the main contributor to accelerating research, like cancer research happens faster with more patients and funding unlike our rare diseases. I think it’s also really nice to see that the international collaboration is paying off. For IGOS, we are now doing a large genetic study to investigate which genetic variants are associated with GBS.
Dr. Fehmi: We need to better select specific patient groups i.e those that don’t respond to treatment, and offer enrollment in clinical trials using immune therapies we know are effective from anecdotal evidence.
Relevant Resources
Centers of Excellence: https://www.gbs-cidp.org/support/centers-of-excellence/
Doctor to Doctor Consult: https://www.gbs-cidp.org/doctor-to-doctor/
Find our Awardee’s Research Here: https://pubmed.ncbi.nlm.nih.gov/
Visit our Research Portal Here: https://www.gbs-cidp.org/research-portal/
Other Articles You May Like

GBS|CIDP Foundation Partners with UNITAR to Advance Global Plasma Access
The Foundation is proud to officially partner with United Nations Institute for Training and Research…

Speaker Series: Estrangement & Isolation, Chronic Illness
Living with a chronic illness can affect much more than physical health—it can also impact…
GBS|CIDP Legislative Agenda 2026 | Advocacy Priorities
Support Robust Research Funding Currently, there is no cure for GBS, CIDP, or MMN. Patients…